|
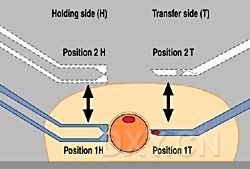
The number of infertile couples has increased in recent years and is now estimated at 15–20% of all couples worldwide. Since its introduction into reproductive medicine in 1978 [1], in vitro fertilization has been considered a successful method of treating tubal sterility. With increasingly intensive diagnosis of both partners, certain aspects of male subfertility are coming to the forefront. Nowadays almost 50% of insterility in couples can be attributed to male subfertility [2]. Intracytoplasmatic sperm injection (ICSI) has raised hopes that these couples can have children of their own. In the meantime this method of treating male subfertility has achieved a breakthrough [3] and is gaining in importance. It is establishing itself as the preferred method of treatment in the field of assisted reproduction, following numerous pregnancies and births [4]. Preparation for ICSI involves obtaining an oocyte by means of follicle aspiration, removal of the cumulus cells and of the corona radiata and preparation of semen in accordance with the Mini Swim-Up process [5] or other preparation procedures [6]. Thereafter, one sperm is injected into this oocyte with a thin glass capillary (pipette). If fertilization has occurred, the embryo is transferred into the uterus 48 hours after microinjection. For the microinjection process described, Eppendorf® offers ideal tools for easing the workload: the micromanipulator TransferMan, used for moving the holding capillary, and a second micro-manipulator TransferMan for transferring the sperm. The actual holding of the oocyte is carried out using CellTram Air, and CellTram Oil is used for transferring the sperm. Operating TransferMan, by means of four self-explanatory keys, is extremely simple. For every TransferMan, two spatial coordinates are defined and stored. The capillary can be moved easily in any direction (x y z) by means of a joystick. By simply pressing the joystick button, the capillary can repeatedly assume one of the pre-programmed positions. Sensibly, a point in the focal plane is chosen for the holding side at which the oocyte can be easily held (position 1 H) and the sperm can be easily injected with the second TransferMan (position 1 T). For both manipulators/ capillaries, a point outside the drops in the overlay oil (Fig. 1) is advisable for position 2 (H and T).
Fig. 1 Injection into oocyte, schematic The method of procedure is as follows: The transfer capillary and the holding capillary are directed at the focal plane and the positions are stored as Pos. 1 (T and H). Similarly, the positions in the overlay oil are defined as Pos. 2 (T and H). Sperm and ova are put onto the petri dish in several drops of oil. By simply pressing the joystick button, the transfer capillary (inner diameter approx. 4–5 µm) is lowered to position 1 T. Magnified x20 times, a sperm cell is immobilized by means of a quick movement of the transfer capillary across the tail, or by pressing the tail of the sperm cell against the bottom of the dish until it stops moving. The sperm cell is aspirated, tail first into the transfer capillary by rotating the knob of the CellTram Oil. By pressing the joystick button, the transfer capillary, which now contains the sperm cell, is moved up into the overlay oil. The petri dish is moved in order to visualize an oocyte in one of the drops surrounding the sperm medium. The oocyte is brought into focus. With the second TransferMan in position 1 H and simultaneous rotation of the knob of the CellTram Air, the oocyte is held with the holding capillary (inner diameter approx. 20 µm). Magnified x10 times, the oocyte is turned with the aid of the transfer capillary, which has been lowered again (position 1 T), until the polar body comes to rest either above (12 o’clock) or below (6 o’clock). This requires the under-pressure on the CellTram Air to be slightly varied. In this position, the oocyte is held with the holding capillary by turning the knob of the CellTram Air. Then the capillaries and the oocyte, (magnification x40) are sharply focussed, the sperm cell in the transfer capillary is brought to the tip by rotating the knob of the CellTram Oil. By moving the joystick slightly, the transfer capillary is carefully pushed through the zona pellucida and the oolemma into the ooplasm at 3 o’clock. The oocyte should be pricked in the middle, so that the oolema membrane is broken gently and atraumatically. If this is not immediately successful, it is aspirated until the membrane perforates. The sperm cell is then injected. In order to introduce only one minimal volume of the medium and PVP solution, or none at all, into the cytoplasm, the transfer capillary is withdrawn gently after the head of the sperm cell has left the pipette tip and is no longer injected.
Fig. 2 Injection into oocyte The injected oocyte is released from the holding capillary. Both capillaries are moved to position 2 by pressing the joystick button. Literature [1] Steptoe PC, Edwards RG (1978) Birth after reimplantation of a human embryo. Lancet ii:366 We would like to thank Dr. S. Al Hasani, Clinic for Gyniatrics and Tocology, Medical University of Luebeck, Ratzeburger Allee 160, D-23538 Luebeck, Germany, for his support in the development of our ICSI workplace. |
→如果您认为本词条还有待完善,请 编辑词条
上一篇ELECTROPORATION OF ES CELLS AND ISOLATION OF H/R CLONES 下一篇DNA from Tail Biopsies
词条内容仅供参考,如果您需要解决具体问题
(尤其在法律、医学等领域),建议您咨询相关领域专业人士。
0
收藏到: